
Published August 15, 2017
Horner’s Syndrome: A Positive Apraclonidine Test—Now What?
Diagnosis isn’t the challenge—finding the cause is.
Practitioners can confirm a case of suspected Horner’s syndrome through in-office pharmacological testing in a straightforward manner, but differentiating benign from life-threatening causes can pose a significant challenge. Symptoms and signs, along with a thorough patient history and review of systems, can help the clinician localize a potential causative lesion and, in turn, help direct neuroimaging studies and subsequent referral to an appropriate specialist.
 |
| Multiple pulmonary pathologies—such as lung cancer in this patient’s case—can cause Horner’s syndrome. Click image to enlarge. |
Beyond the Cookbook
All optometrists can recite the classic triad of –osis findings associated with Horner’s syndrome: ptosis, pupillary miosis, facial anhidrosis. Some cases can also include heterochromia of the iridies if the syndrome developed prior to two years of age.1-8 Often, patients will display a dilation lag in dim illumination; that is, the affected pupil will slowly dilate and the anisocoria will diminish after several minutes in a dark room.
However, not every case of Horner’s syndrome will manifest classically; a “cookbook” approach to diagnosis is insufficient. It is incumbent on the clinician to use every clue in the presentation to suspect Horner’s syndrome may be present. In such cases, the dilation lag may be quite helpful in prompting pharmacologic testing.
Knowledge of the relevant anatomy is critical to localize the cause of confirmed Horner’s syndrome.
A three-neuron arc provides sympathetic innervation to the eye.1-8 Horner’s syndrome is an interruption along this oculosympathetic pathway, between its origin in the hypothalamus and the ipsilateral dilator muscle of the eye.1-8 The first-order neuron originates in the hypothalamus, where it descends through the brain stem to the ciliospinal center of Budge, between C8 and T4 of the spinal cord.1-9 At this level, it synapses with the second-order neuron whose preganglionic cell bodies give rise to fibers that exit the spinal cord through the ventral spinal root; from here, they pass over the apex of the lung and enter the sympathetic chain in the neck, where they synapse in the superior cervical ganglion.1-8
There, in the superior cervical ganglion, cell bodies of third-order neurons give rise to postganglionic fibers that travel with the internal carotid artery through the cavernous sinus towards the eye.1-9 These postganglionic fibers form the long posterior ciliary nerves, which course with the branches of the fifth cranial nerve to innervate the iris dilator muscle, Müller’s muscle and lacrimal gland.1-9
Additionally, postganglionic sympathetic fibers, responsible for facial sweating, follow the external carotid artery to the sweat glands of the face.1-8
Pharmacological Testing
Historically, topical liquid 10% cocaine was used to identify the presence of Horner’s syndrome, and topical hydroxyamphetamine was used to aid in localizing a postganglionic lesion.4-8,10 Today, these agents are not practically available; instead, the diagnosis of a suspected Horner’s syndrome can be confirmed by pharmacological testing with apraclonidine 0.5% or 1%.4-8,10
In Horner’s syndrome, the affected pupil and levator undergo denervation hypersensitivity.10-15 Apraclonidine is an alpha-2 adrenergic agonist that also acts as a very weak alpha 1-adrenergic agonist; when topically applied in Horner’s syndrome, it causes dilation of the affected pupil and possibly lid elevation, without change to the normal pupil.10-15 These changes are so dramatic that a ‘reversal’ occurs; the normal pupil and lid now appear ptotic and miotic in comparison with the apraclonidine-positive eye.
Although sensitivity of apraclonidine testing is very good, false negative testing with apraclonidine may occur in acute Horner’s syndrome as the test relies on denervation hypersensitivity, which may not have had time to occur.12,13However, there are reports of positive apraclonidine tests within a few hours of the onset of symptoms related to Horner’s syndrome.14,15 Again, if the findings are equivocal but suspicion still high, one must go with clinical intuition and investigate further.
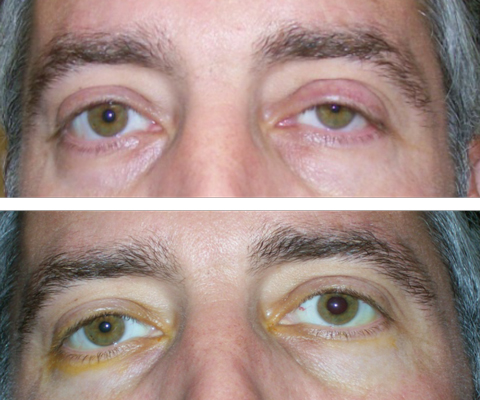 |
| At top, this patient presented with suspected left Horner’s syndrome, pre-apraclonidine testing. At bottom, post-apraclonidine testing led to reversal, confirming the diagnosis.Click image to enlarge. |
Finding the Cause
Apraclonidine testing can easily confirm the diagnosis of Horner’s syndrome, but is unable to localize the lesion. Due to the long course of the oculosympathetic pathway from hypothalamus to the eye, there are multiple locations of potential pathology in Horner’s syndrome.16 Common etiologies include, but are not limited to: carotid artery dissection, aortic dissection, trauma, demyelinating disease such as multiple sclerosis (MS), tuberculosis, sarcoidosis, cluster headache, Pancoast syndrome, herpes zoster, giant cell arteritis (GCA) and malignancy.1-8,16,17 A careful physical exam and patient history can help guide imaging studies to aid in determining the location of the lesion.16
Once Horner’s syndrome is diagnosed (such as with a positive apraclonidine test), a directed evaluation is always preferable to non-specified testing. This is where knowledge of anatomy, symptoms and associated finding becomes crucial. For example, if there is a positive history of neck or facial pain, headache, recent neck trauma, ipsilateral vision loss or transient numbness or weakness on the opposite side of the body, an asutute clinician should suspect acute carotid artery dissection and order emergent neuroimaging.18-22
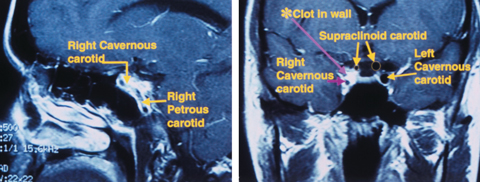
In cases caused by internal carotid artery dissection, significant risk exists for major stroke within the first two weeks of onset.18-20 Computed tomography (CTA) or magnetic resonance angiography (MRA) of the neck and cervical spine, which must include Circle of Willis and the orbits down to the level of the aortic arch (T4-T5), which includes the carotid arteries and intracranial vessels as well as lung apices, is recommended.16,22 For cervical arterial dissections, CTA is the preferred imaging modality as, though MRI shows resolution with high contrast, it has lower temporal and spatial resolution.23
In cases involving acute pain with onset of Horner’s syndrome, the patient requires emergency referral with imaging performed on the same day as clinical evaluation.16 Preferably, practitioners should not try to obtain this imaging themselves; rather, they should send the patient directly to the emergency room with detailed notes on the diagnosis of Horner’s syndrome and the clinical suspicion of carotid dissection. If they have just performed apraclonidine testing on the patient and they note apparent pharmacologic ‘reversal’ of the Horner’s syndrome, they must explain everything clearly in the referral notes so that the emergency room physicians focus on the correct anatomical side.
Carotid artery dissection, which affects the third-order neuron, can result from relatively minor trauma, or can occur spontaneously in patients with histories of connective tissue disease such as Ehlers-Danlos syndrome, Marfan’s syndrome or those with long-standing hypertension.1-8,24
In patients with histories of tobacco use, ipsilateral shoulder or arm pain or muscle weakness of the hand and arm, localization could lead to a lesion at the apex of the lung.25,26 As the oculosympathetic plexus courses over the apex of the lung via the second-order neuron, multiple pulmonary pathologies can cause Horner’s syndrome. For instance, Pancoast syndrome is a malignancy of the superior pulmonary sulcus most often caused by non-small cell lung carcinoma.25 Pancoast tumor has a rapid and high mortality rate.25
Neuroradiological evaluation, typically including MRI of the chest and neck with and without contrast, and physical examination, often performed in concert with an internist, may lead to other chest and lung pathologies, including sarcoidosis or tuberculosis.16,26 Suspicion of cancer warrants a referral to primary care.
After Apraclonidine: The Next Steps
Once the apraclonidine test is positive for Horner’s syndrome, here are the next four steps in your clinical workup:
Step 1: Probe the patient’s history to see if the lesion can be localized. Any head, neck or eye pain can be suspicious for internal carotid artery dissection. Facial weakness or numbness generally localize to abnormalities within the middle cranial fossa. Tobacco history can cause concern for cancer at the lung apex. Other lung pathology may indicate sarcoidosis or tuberculosis. Dermatologic vesicles and neuralgia can identify zoster as a cause. Cluster migraines also can cause Horner’s syndrome. Thus, a physical examination and history, often done in concert with an internist, help dictate management.
Step 2: Look for other neurologic signs. Cranial nerve VI palsy in association with Horner’s identifies cavernous sinus as area of interest, but does not rule out a brain stem lesion. Current or past history of optic neuritis can indicate MS.
Step 3: Look at the age of the patient. Young people can suffer from MS and older people can suffer from stroke. Always assess GCA risk in patients older than 60.
Step 4: Obtain the appropriate imaging. It’s best to image the area of suspicion as identified above. If that is unrevealing, the patient must be imaged from chest to head including MRA or CTA of neck for carotid dissection, MRI of brain with and without contrast with attention to middle cranial fossa and cavernous sinus, and chest/neck MRI or CT to include the brachial plexus and cervical spine. Non-targeted evaluations are often non-productive, but still recommended to rule out treatable pathology. Unless the patient has an emergency situation regarding carotid dissection, consider referring to a primary care physician or neurologist for an overall health evaluation with consideration for these conditions.
|
Other Neurological Signs
In patients presenting with abducens (cranial nerve VI) palsy in addition to Horner’s syndrome, clinicians should pay attention to the cavernous sinus.5,27The oculosympathetic plexus travels with the abducens nerve within the cavernous sinus.5,27,28 MRI of the brain with and without contrast, with attention to the middle cranial fossa and cavernous sinus, is warranted.
However, lesions of the first-order neuron including brain stem lesions in Horner’s syndrome may also cause abducens nerve palsy, so additional clinical signs and symptoms can aid in localization. Patients with first-order neuron Horner’s syndrome typically present with widespread neurological symptoms including contralateral hemiparesis, contralateral hypesthesia and hypohidrosis of one side of the body.16,29 Pontine lesions such as stroke may additionally result in dizziness, nausea and difficulty swallowing.29,30 In cases of nystagmus, vertigo and vomiting—in addition to Horner’s syndrome, lateral medullary infarction or Wallenburg syndrome—may be present.29 Horner’s syndrome with trochlear (cranial nerve IV) palsy suggests the dorsal mesencephalon is an area of interest for clinicians to investigate.29
In cases of Horner’s syndrome, consider the age of the patient. In younger patients, demyelinating disease, including MS, can be a potential cause of Horner’s syndrome. In older patients, stroke, zoster and GCA are etiologies that practitioners should consider.21,32
When no diagnostic clues are identified following a complete clinical examination, a non-targeted evaluation, including imaging of the upper chest, neck, and brain, must be performed.16,17,22 MRI of the neck and chest including the lung apex, MRA or CTA of the neck and cervical spine, and MRI of the brain, with attention to the middle cranial fossa, is recommended. Imaging centers may have a protocol for dealing with Horner’s syndrome to ensure that proper studies are done. In many cases, even with extensive imaging, an underlying cause may not be determined.9,16,17
With any radiology referral, it is important to provide the neuroradiologist with all available localizing information available—including the anatomical location of Horner’s syndrome—to allow for clinical-radiologic correlation.11 Remember, a neuroradiologist cannot help you if you do not:
- order a scan,
- order the correct scan, and
- specify what you are looking for.
Once Horner’s syndrome has been identified with a positive apraclonidine test, the real work begins. Optometrists must use their knowledge of anatomy and rely on the history and clinical exam to determine potential causes, send to an emergency room when appropriate, order necessary diagnostic testing and comanage with other medical specialists when necessary.
Dr. Steen is an attending optometrist and assistant professor of ocular pharmacology at Nova Southeastern University’s College of Optometry.
Dr. Sowka is a professor at Nova Southeastern University.
View Footnotes
No comments:
Post a Comment